
Peptides and Joints: Turning Back the Clock
Executive Summary
Joint discomfort is one of the biggest roadblocks for athletes over 35, often forcing them to scale back training or abandon the activities they love. Aging reduces the body’s ability to maintain cartilage, tendons, and joint lubrication, while hormone shifts and accumulated injuries add to the burden. Recent research suggests peptides may not only ease symptoms but actively support repair and regeneration—raising the body’s “recovery threshold” and enabling healing that might otherwise stall. Combined with energy-boosting agents like NAD⁺ and MOTS-c, peptides may represent a path to extend athletic performance and joint health well beyond what was once possible.

Table of Contents
Why Joint Health Declines After 35
As athletes age, their bodies undergo systemic changes that directly affect joint health:
- Degeneration: Cartilage thins, synovial fluid decreases, tendons stiffen.
- Inflammation: Microtraumas and overuse fuel chronic low-grade inflammation.
- Hormones: Declining testosterone and estrogen slow collagen synthesis, reduce joint lubrication, and weaken muscle support around joints.
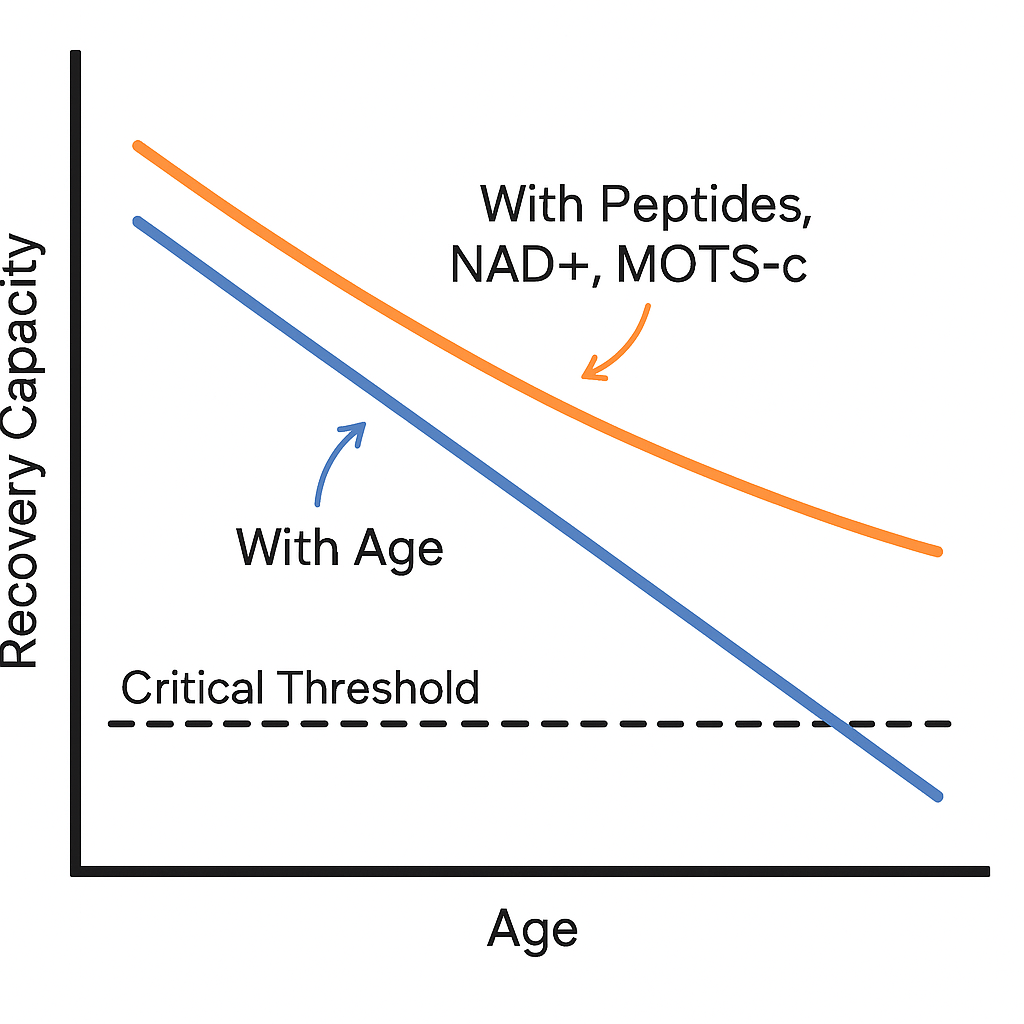
- Recovery Threshold: The body can only allocate so much energy to repair and regeneration. Aging lowers this threshold, meaning that when training loads, old injuries, or systemic stress pile on, healing may not “fit into the budget”—leaving injuries to linger or worsen.
Peptides: Raising the Recovery Threshold
Peptides work by signaling the body to prioritize repair processes that aging often leaves unfinished:
- BPC-157 directs resources toward angiogenesis, tendon-to-bone healing, and joint capsule repair (Sikiric et al., 2020).
- TB-500 (Thymosin Beta-4) mobilizes progenitor cells and enhances tissue flexibility (Goldstein et al., 2012).
- GHK-Cu stimulates synthesis of collagen and glycosaminoglycans, directly supporting cartilage and joint lubricity (Pickart et al., 2015).
- CJC-1295 + Ipamorelin increases pulsatile growth hormone release, raising IGF-1 and directly fueling connective tissue rebuilding (Khorram et al., 2001).
By amplifying repair signaling, peptides raise the recovery threshold, making it possible to complete repairs that previously stalled due to energy or hormonal limitations.
Low Testosterone and Joint Pain: A Classic Marker
Low testosterone is increasingly recognized as a driver of joint discomfort in aging men.
- Reduced collagen synthesis weakens tendons and cartilage (Bhasin et al., 2001).
- Decreased muscle mass lessens shock absorption and stability around joints.
- Increased inflammation is linked to hypogonadism and low T states (Mohamad et al., 2019).

Athletes with unexplained joint pain, especially in the absence of structural injury, often discover low testosterone as an underlying factor. Peptides that support GH/IGF-1 (like Ipamorelin or CJC-1295+Ipamorelin) can help mitigate this, but in many cases, optimizing testosterone itself must be part of the plan.
The Energy Layer: NAD⁺ and MOTS-c
Even with optimal signaling, healing requires raw energy. Aging athletes often lack the mitochondrial horsepower to fully repair tissue.
NAD⁺ Decline with Age
NAD⁺ (nicotinamide adenine dinucleotide) is essential for energy production and DNA repair. Levels decline dramatically with age:
- By middle age (40–60 years), NAD⁺ levels fall by ~50% compared to youth (Yoshino et al., 2018).
- In individuals over 70 years, NAD⁺ may be reduced by as much as 65–80% in some tissues (Massudi et al., 2012).
This decline limits the ATP available for tissue repair, contributing to stalled healing and chronic inflammation.
MOTS-c: The Mitochondrial Booster
- Improves metabolic efficiency by activating AMPK (Lee et al., 2015).
- Reduces inflammatory stress on joints.
- Increases recovery capacity after heavy training loads.
Together, NAD⁺ and MOTS-c raise the recovery threshold by both improving energy availability and reducing repair bottlenecks—allowing peptides like BPC-157 and GHK-Cu to do their work more effectively.
Ipamorelin vs. CJC-1295 + Ipamorelin
Although often mentioned together, these represent distinct approaches:
- Ipamorelin (solo): A growth hormone secretagogue used for daily, shorter-term boosts. Known for its clean side-effect profile, minimal impact on cortisol/prolactin, and flexible cycling (Raun et al., 1998).
- CJC-1295 + Ipamorelin: Combines a GHRH analog (CJC-1295) with a GHRP (Ipamorelin) to create synergistic, pulsatile GH release. Often used in medium to longer cycles for more robust IGF-1 increases and connective tissue support (Khorram et al., 2001).
Both enhance collagen synthesis and joint repair, but the combination generally delivers greater anabolic and recovery benefits.
General Protocol Guidance (Research Context Only)
⚠️ These protocols are cited from research/athletic community use, not medical recommendations.
- BPC-157: 250–500 mcg daily (localized near injury if subcutaneous). Cycles: 4–6 weeks.
- TB-500: 2–5 mg weekly (split into 2 doses). Cycles: 4–6 weeks.
- GHK-Cu (injectable): 2–5 mg daily for 2–4 weeks.
- Ipamorelin (solo): 100–200 mcg 2× daily (AM fasted, PM pre-bed). Cycles: 8–12 weeks, 2–4 weeks off.
- CJC-1295 + Ipamorelin: 100 mcg of each, 2× daily (AM fasted, PM pre-bed). Cycle: 8–12 weeks, 2–4 weeks off.
- MOTS-c: 10–15 mg 2–3× weekly. Cycle: 4–6 weeks.
- NAD⁺: 100–300 mg weekly (IV or subcutaneous), or microdosing protocols.
Practical Benefits for Athletes 35+
- Healing of injuries that previously stalled.
- Reduction of low-T–related joint discomfort.
- Enhanced tendon flexibility and smoother joint movement.
- Accelerated recovery timelines by raising the body’s repair capacity.
- Synergistic support when peptides are combined with NAD⁺ and/or hormone optimization.
Final Thoughts
Joint decline is not an inevitable sentence for athletes over 35. By understanding recovery thresholds—and how peptides, hormones, and mitochondrial enhancers can raise them—it becomes possible to repair injuries and maintain joint function long past the supposed limits of aging. For those committed to staying in the game, this combined approach represents one of the most promising frontiers in performance longevity.
Disclaimer: These compounds are not FDA-approved for joint health, and most evidence comes from animal studies or limited human trials. Their use should be considered experimental and only undertaken with full awareness of regulatory and medical risks.
References
- Sikiric P, et al. Stable gastric pentadecapeptide BPC 157: A therapy for the future? World J Gastroenterol. 2020;26(25):3222-3250.
- Goldstein AL, et al. Thymosin β4: A multifunctional regenerative peptide. Ann N Y Acad Sci. 2012;1269(1):9-19.
- Pickart L, et al. GHK peptide as a natural modulator of multiple cellular pathways in skin regeneration. BioMed Res Int. 2015;2015:648108.
- Khorram O, et al. Administration of CJC-1295, a long-acting GHRH analog, results in sustained, dose-dependent increases in GH and IGF-1. J Clin Endocrinol Metab. 2001;86(12):5732-5739.
- Bhasin S, et al. Testosterone and skeletal muscle. Endocr Rev. 2001;22(4):389-424.
- Mohamad NV, et al. The relationship between testosterone and inflammation: A review. Malays J Med Sci. 2019;26(1):5-18.
- Yoshino J, et al. NAD⁺ intermediates: The biology and therapeutic potential of NMN and NR. Cell Metab. 2018;27(3):513-528.
- Massudi H, et al. Age-associated changes in oxidative stress and NAD⁺ metabolism in human tissue. PLoS One. 2012;7(7):e42357.
- Lee C, et al. The mitochondrial-derived peptide MOTS-c promotes metabolic homeostasis and reduces obesity and insulin resistance. Cell Metab. 2015;21(3):443-454.
- Raun K, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552-561.